
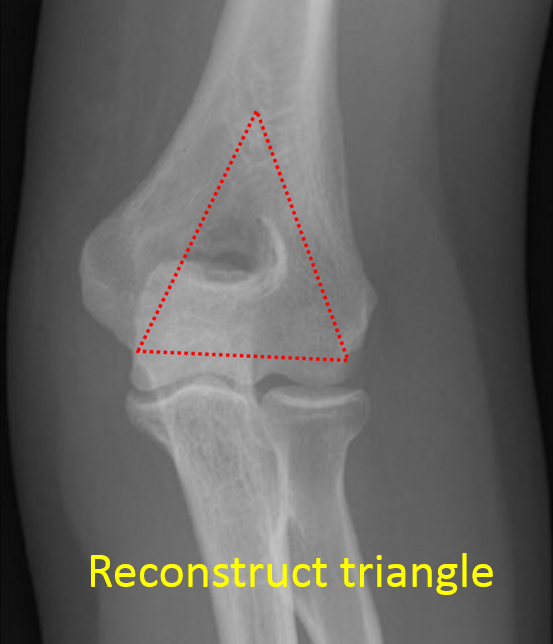
Today, we’re going to talk about Elbow Reconstruction in trauma cases. The main principle which we have to keep in mind when reconstructing the elbow is- stable internal fixation of articular surface & also stable internal fixation of the articular segment to the metaphysis & diaphyseal fragments.
Clinical Presentation
- 34 year old male
- History of RTA
- Presented on the day of Injury
- Pain and swelling over left elbow with abrasion and bleeding from the wound
- Difficulty in elbow movement
- Co-morbidities – None
Investigations
- X-ray of the suspected region- pelvis/chest/spine screening/limbs.
- X-ray of affected region- anteroposterior/lateral/traction views (author preference)
- CT scan of elbow (cost constraint)- gold standard
- Blood workup for surgical fitness
- Additional test as required for co-morbidities if any

Clinical Evaluation
- Soft tissue envelope
- Neurological status distal to injury
- Vascular status distal to injury
Goal and Principle of Surgical Fixation
Goal of treatment
To achieve stable fixation, union of fracture fragments with restoration of function of elbow.
Principles of fixation
- Anatomical reduction of intra-articular fragments
- Preservation of blood supply
- Stable fixation
- Early and safe mobilization
Importance of Surgical Plan
- Surgeon needs to pre-formulate a surgical fixation plan and the necessary approach for adequate exposure.
- In addition to the above planning, a backup/contingency plan also needs to be formulated in such complex trauma cases.
Surgical Issues
- Principle of stable fixation constitute
- Stable internal fixation of articular surface
- Stable internal fixation of the articular segment to the metaphysis and diaphyseal fragment
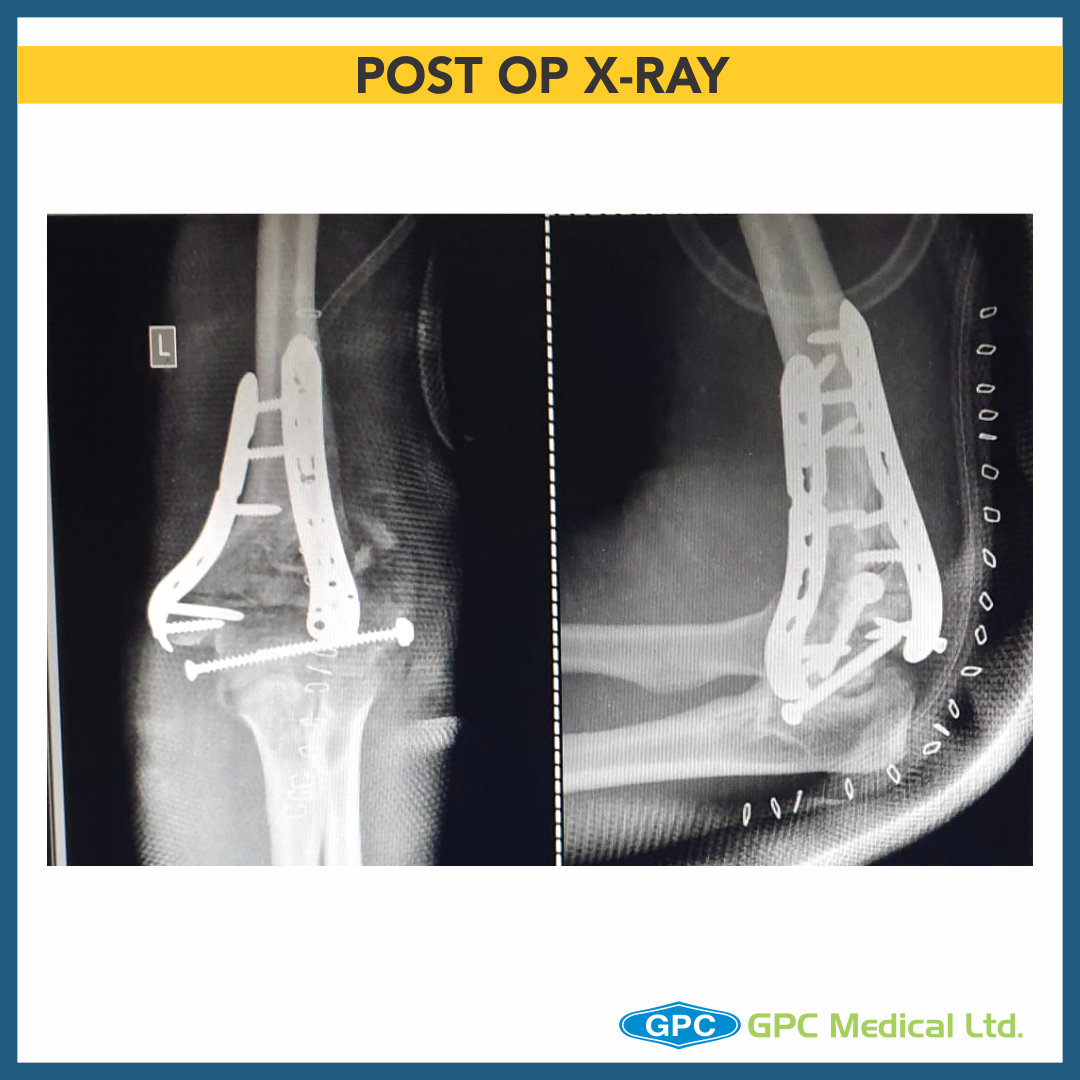
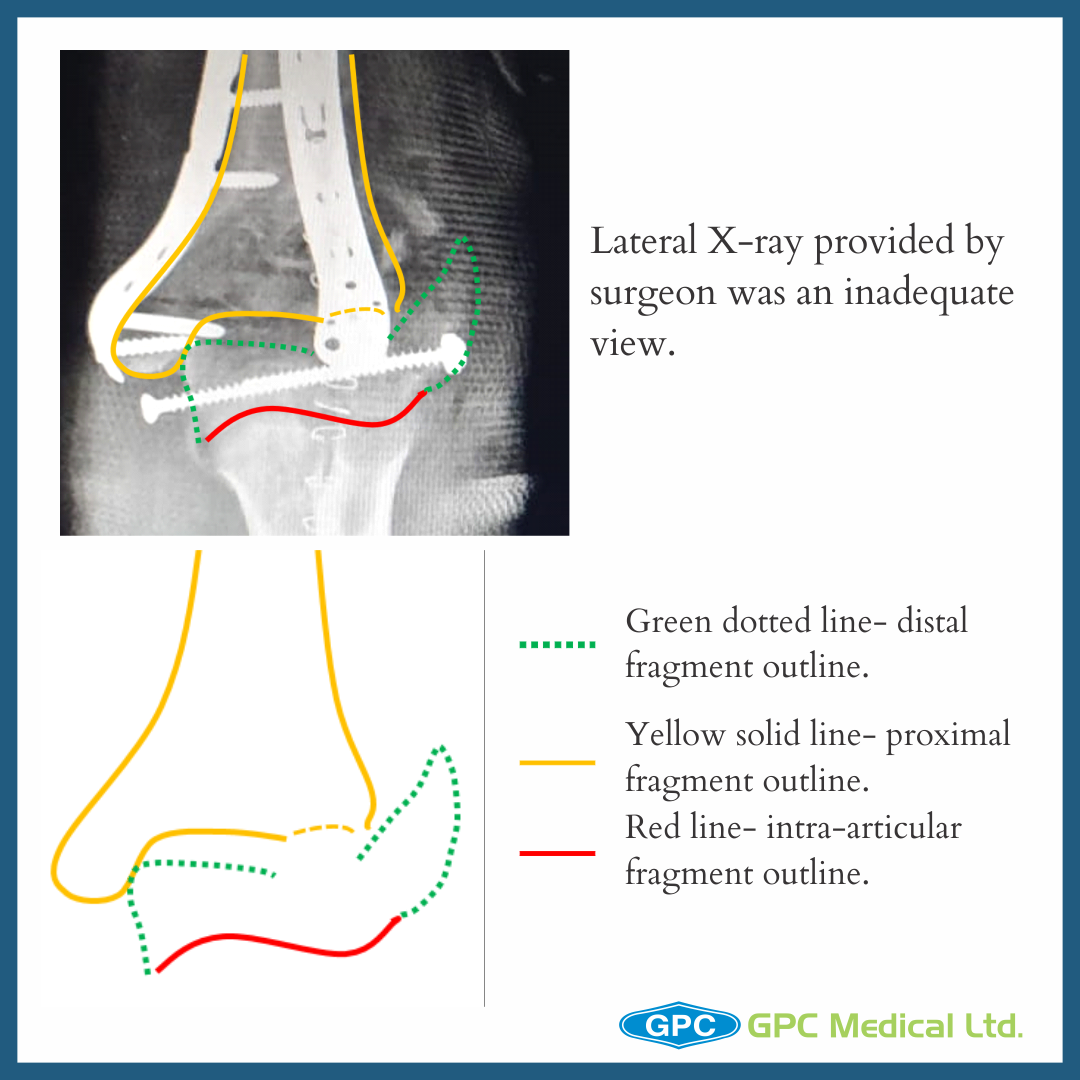
- The surgeon although was able to achieve reduction of the intra-articular fragment, the distal construct was fixed in translation to the proximal construct.
- Different exposures gives good to complete visualization of articular surface
- Choose the exposure depending upon
- Surgical experience
- Type of implant
- Patient factors- skin condition/age/fracture pattern
- Future need of elbow arthroplasty
- Author’s preference
- Olecranon osteotomy (fixation with TBW/ Long screw+ SS wire)
- Byran-Morrey Approach (Triceps-sparing postero-medial approach)
- Midline incision
- Ulnar nerve identified, mobilized and latex loop placed
- Medial edge of triceps and distal forearm fascia elevated as single unit off olecranon and reflected laterally
- Resection of extra-articular tip of olecranon(better visualization, later helps during ROM exercises)
Adequate Visualization on C-arm During Surgery
At 90° flexion: The olecranon overlaps only a small part of the medial joint surface
- If elbow flexion is increased to 110°- free and complete joint surface is seen on lateral radiograph
- It is therefore important to have proper patient positioning allowing elbow movement and facilitate radiography.
Pre-op Counselling
What patients may expect?
- Loss of 15-25° of flexion and extension
- Maintain most of supination and pronation
- Decrease in muscle strength (triceps)
- Implant impingement (especially olecranon fixation implant)
- Complications associated with the procedure
