
Today, we’re going to talk about Tibial plateau fractures & the depressed fragment elevation technique! Anatomic reduction of the fracture & rigid fixation is the key!
CASE 1
Clinical Presentation:
- 60 years female.
- Slip and fall at home.
- Severe pain in right knee with restricted knee ROM and inability to weight bear on right leg.
Radiological Investigation:
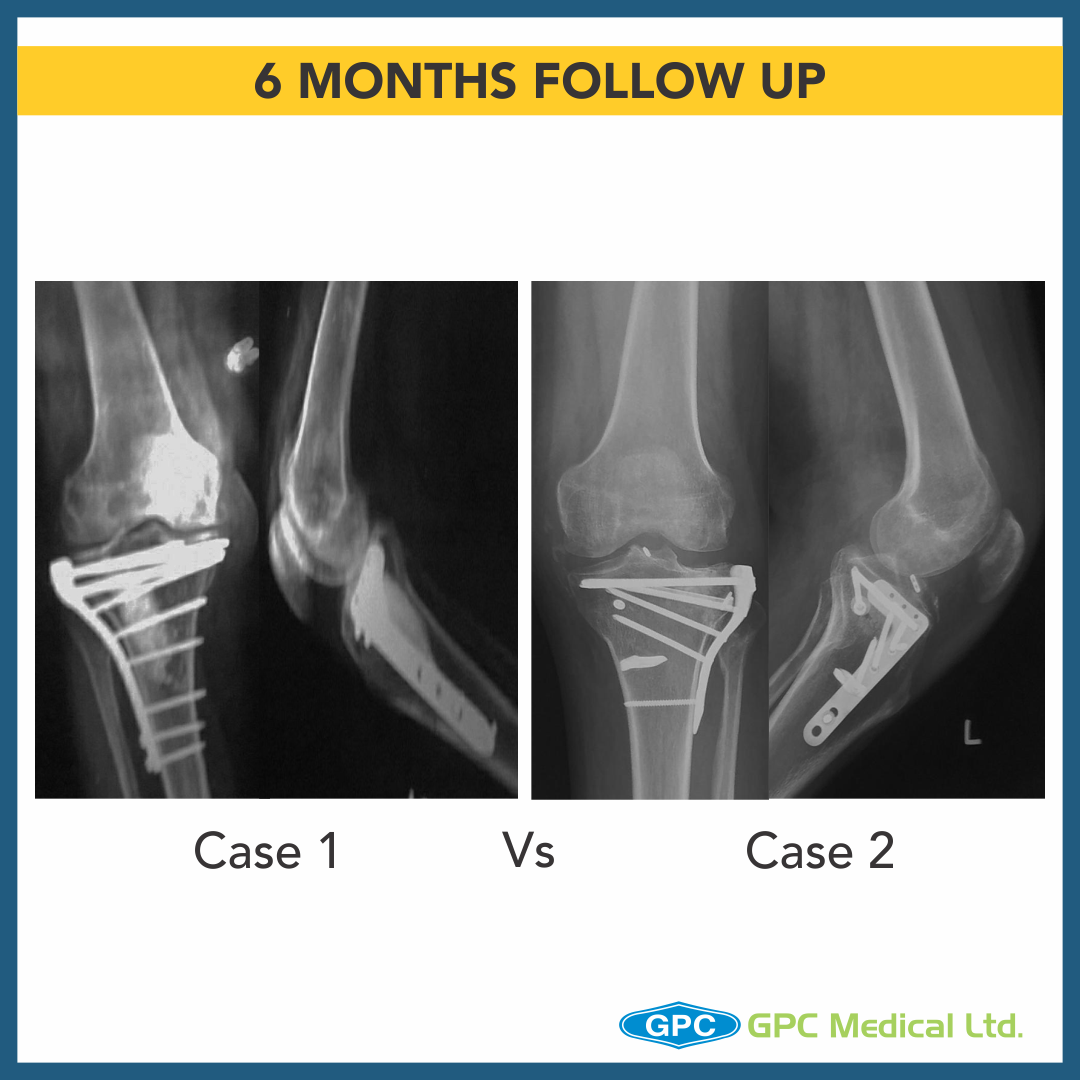
- X-Ray Right knee – Anteroposterior and Lateral Views
Diagnosis:
- Split Depression Lateral Tibial Plateau Fractures (Schatzkers Type 2).

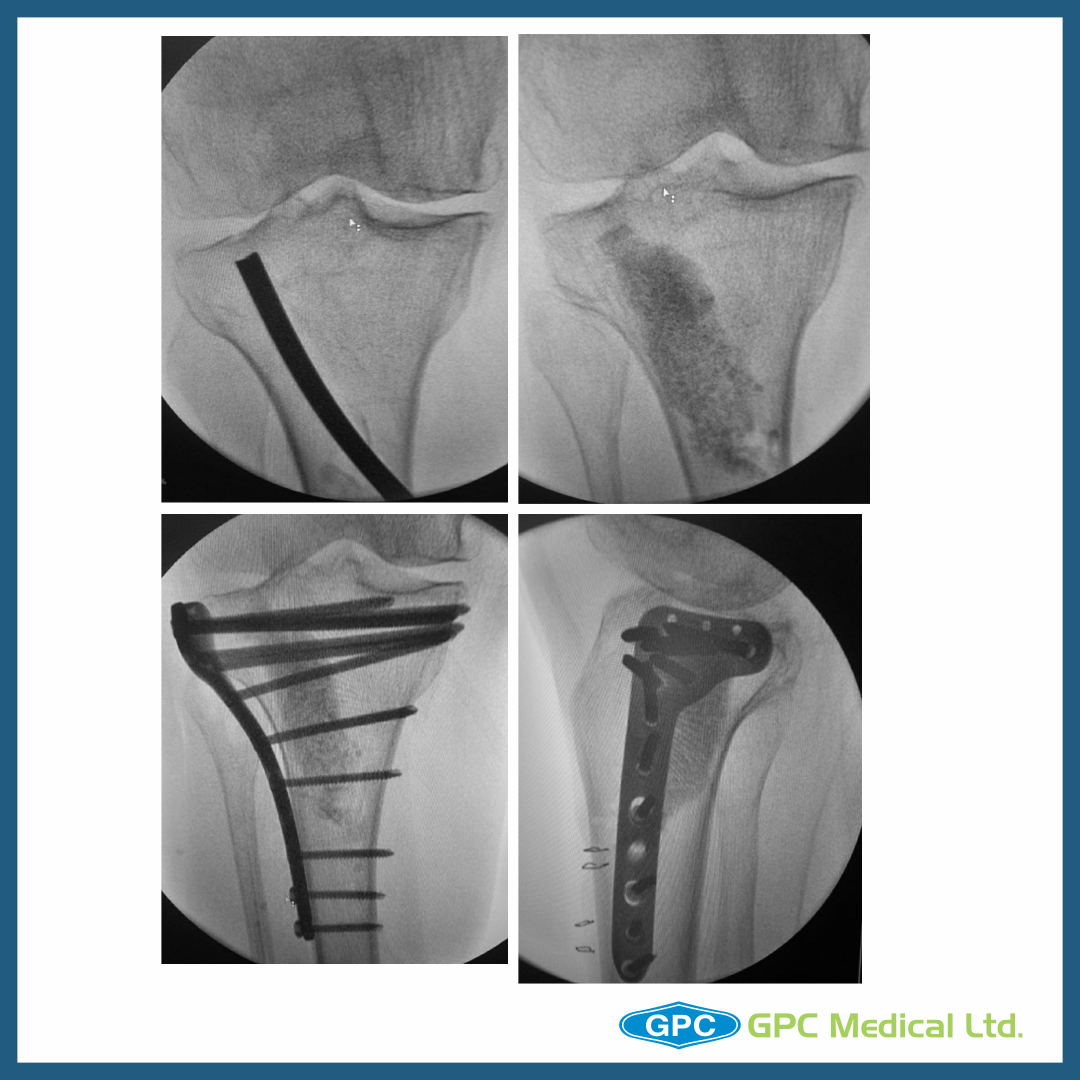
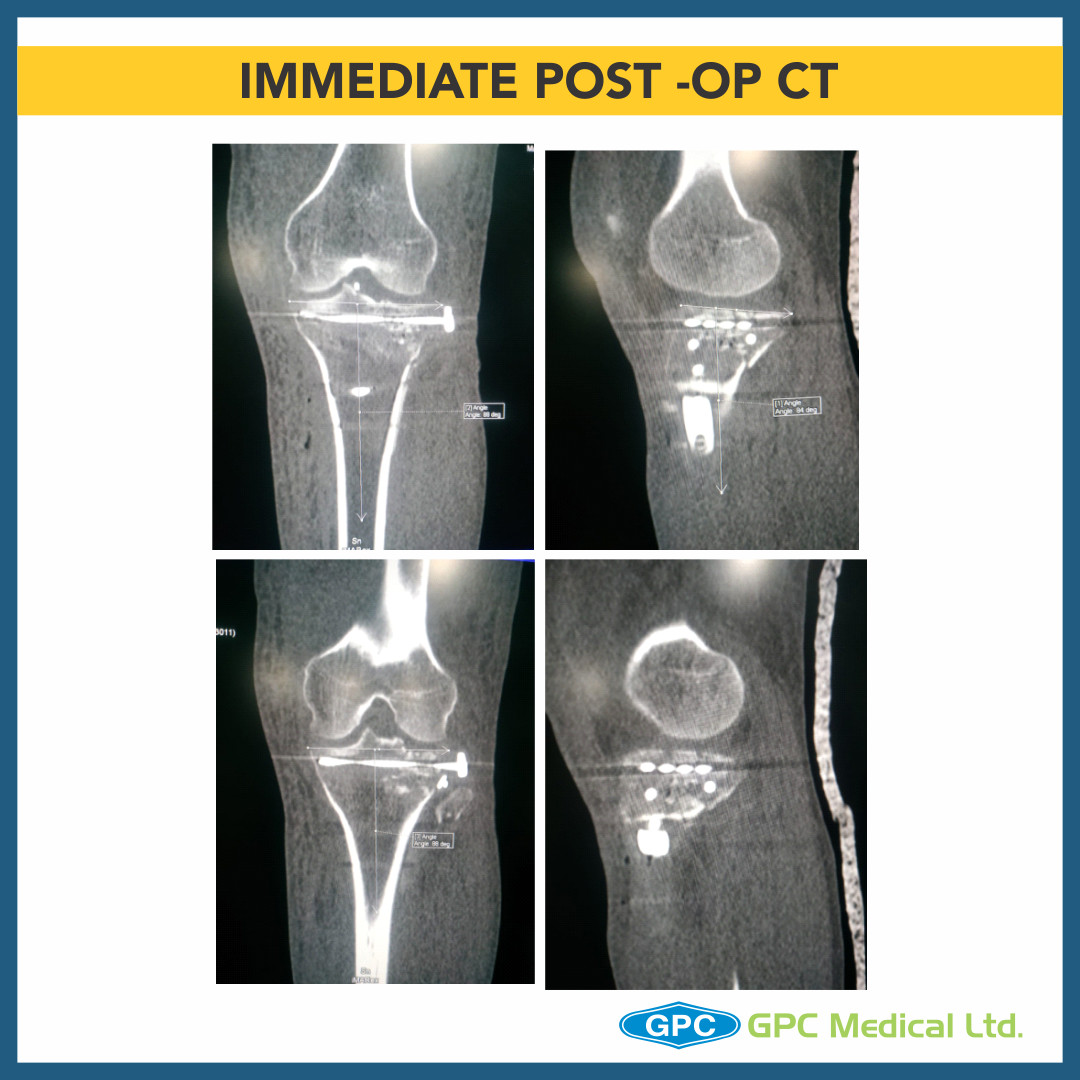
- Intraoperatively under image intensifier depressed fragment is identified in both AP & Lateral views.
- Medial cortical window created.
- Using curved bone punch under image guidance defect is elevated while visualizing in both AP and lateral views with gentle taps/ blows to punch.
- Once satisfactory elevation/ reduction of articular surface is attained, the restored surface is stabilised with k-wire.
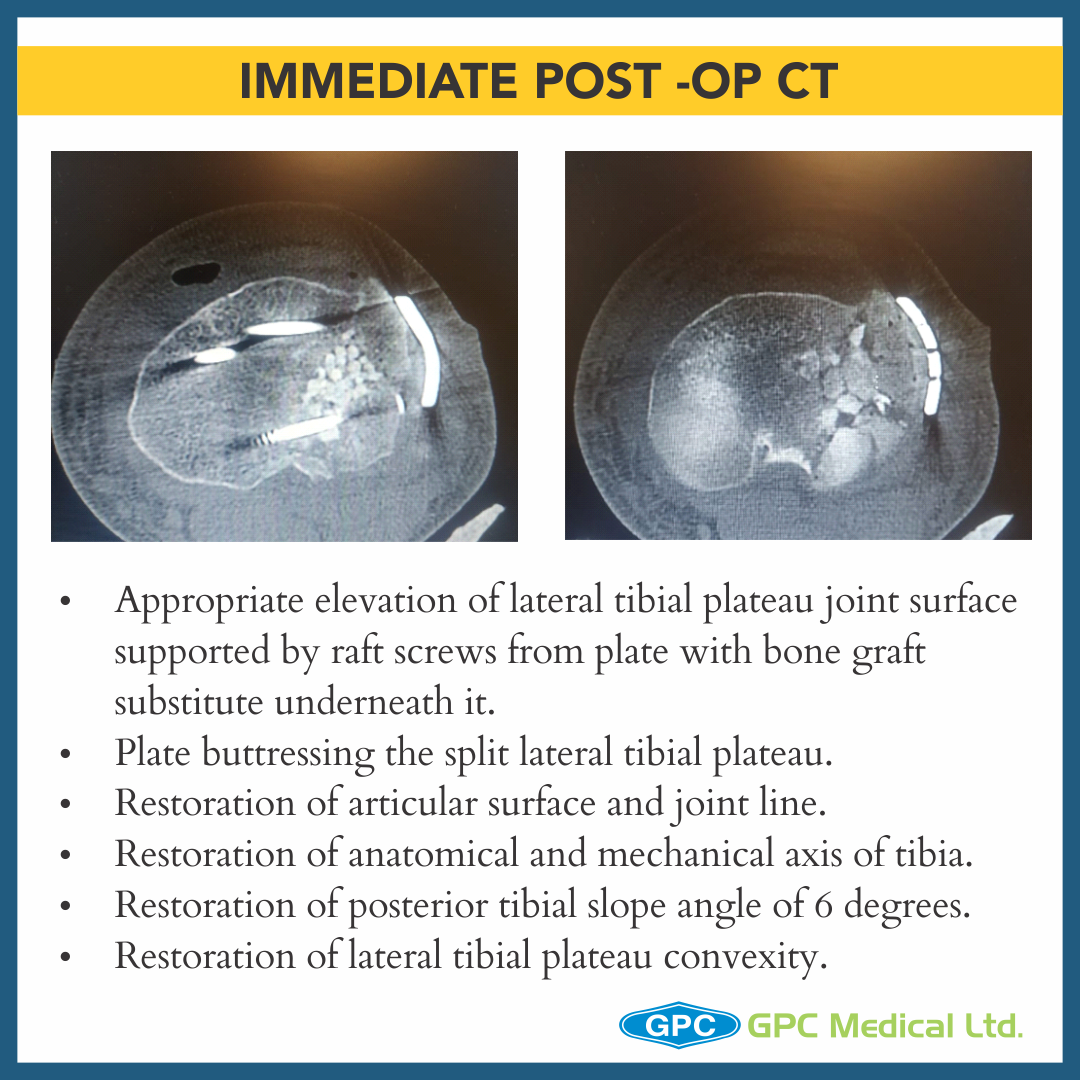
- The defect thus created in metaphyseal region is grafted thus providing subchondral support.
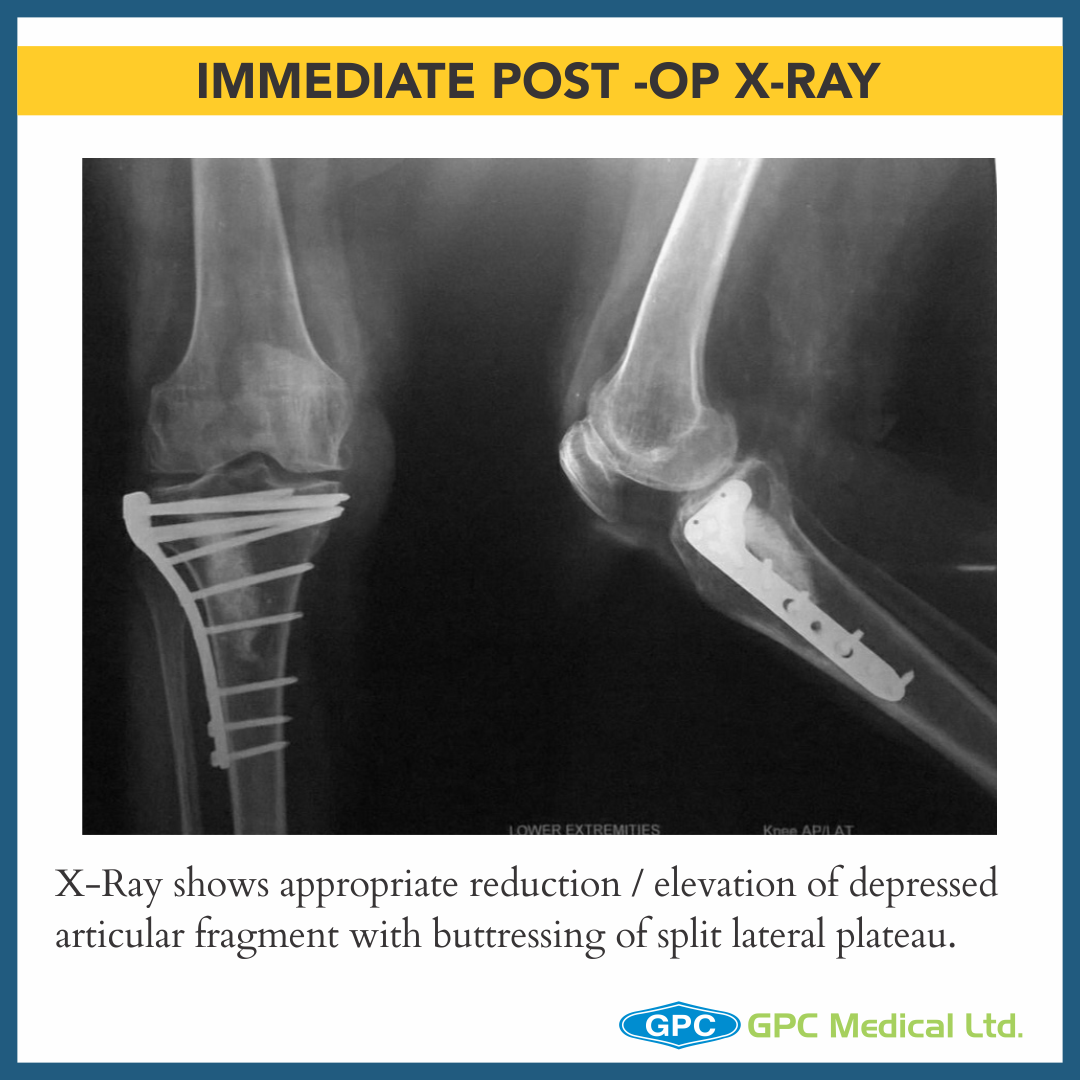
- Finally plating done using MIPPO technique to provide lateral buttress and raft screws providing subchondral support.
CASE 2
Clinical Presentation:
- 39 years male.
- Motor Vehicle Accident.
- Severe pain in left knee with restricted knee ROM and inability to weight bear on left leg.
Radiological Investigation:
- X-Ray Left knee – Anteroposterior and Lateral Views
Diagnosis:
- Split Depression Fracture Lateral Tibial Plateau with Tibial Eminance (ACL attachment) avulsion and MCL Injury


- Intraoperatively under image intensifier depressed fragment is identified in both AP & Lateral views.
- Fracture split is jacked open allowing direct visualisation of depressed joint surface.
- Using punch (here a curette) under image guidance defect is elevated while visualizing in both AP and lateral views.
- Once satisfactory elevation/ reduction of articular surface is attained, the restored surface is stabilised with k-wire.
- The defect thus created in metaphyseal region is grafted thus providing subchondral support.
- Split repositioned, compressed and stabilised with K-wires.
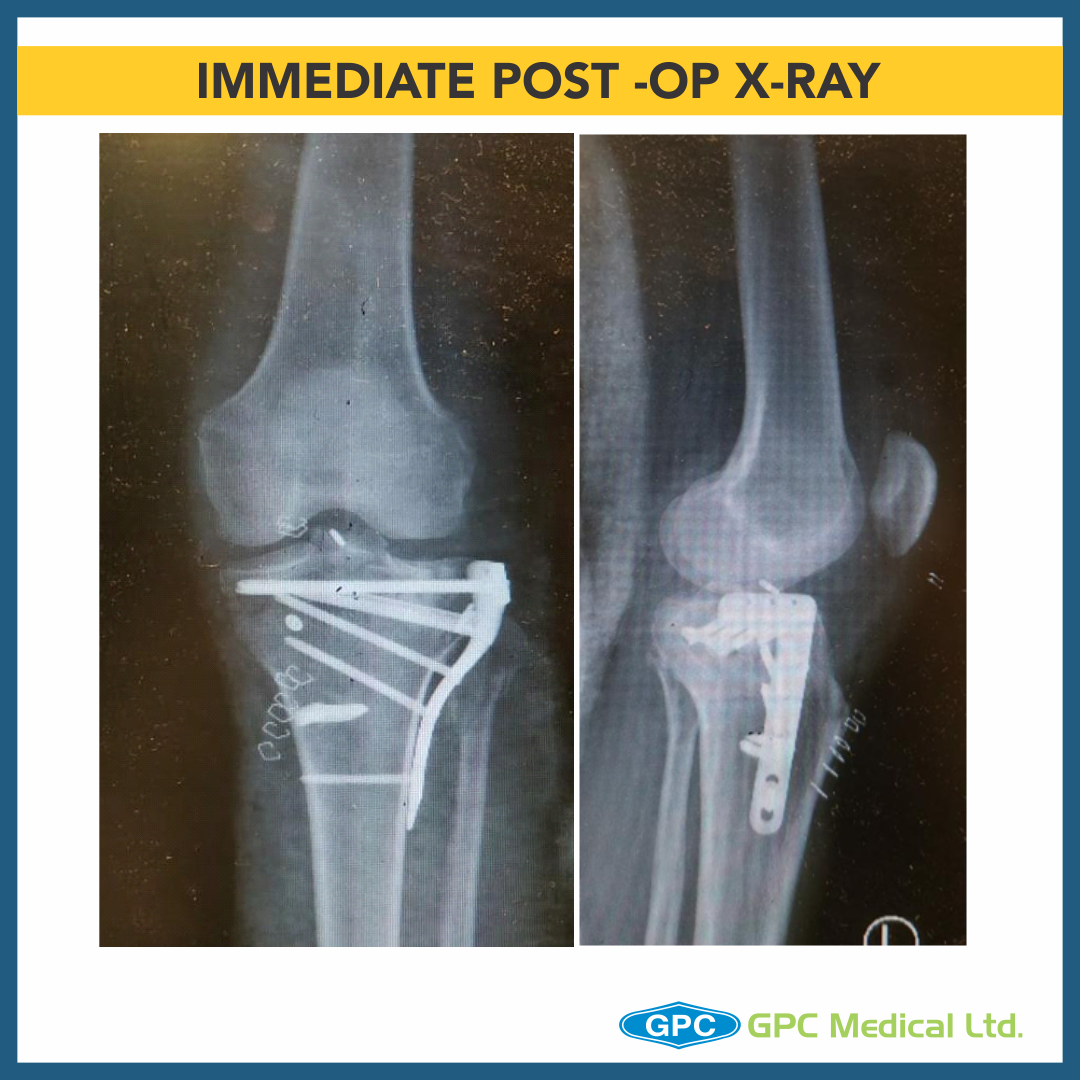
- Finally plating done using MIPPO technique to provide lateral buttress and raft screws providing subchondral support.

- Aulsed ACL attachment/Tibial eminance stabilised, compressed ACL jig under image intensifier and fixed using Mini Tight Rope
- Split posterolateral fragment reduced, stabilised and fixed with 4mm CCS in compression mode, restoring congurity of lateral tibial plateau.
- MCL was intraoperatively found to be avulsed from its tibial attachment site, reenforced with ethibond and fixed using bone staple.
- Thus, managing fracture with associated multi-ligamentous injury in toto.

Surgical Principles and Lacunae in Management
- Principles
- Management for Periarticular Fractures is based on concept of Anatomical reduction of fracture.
- To allow for Primary Bone Healing to happen, Absolute stability and Rigid fixation must be attained.
- Use reduction technique that respects the biological principles of fixation (closed, minimally invasive or open).
- Lacunae
- Failure to restore articular surface anatomically may result in long term post traumatic arthritis.
